June 27, 2021
Updated August 2022
“The vaccines for COVID-19 are safe.” We can’t turn on the television or radio without hearing this assertion over and over. What does it even mean? What is the difference between a treatment that is ‘safe’ and one that is not?
Oxford Dictionary defines “safe” as “Protected from or not exposed to danger or risk.” Merriam-Webster defines it as “free from harm or risk.” To be safe, according to the two leading English dictionaries, means to be free from risk. Of course, there is a low level of risk in everything. Your next meal could kill you due to E. coli poisoning. You could get hit by a car crossing the street tomorrow and become seriously injured. How high must be the degree of risk for an activity to be “risky” or “unsafe”?
The answer to that is entirely personal and subjective. I would never go kayaking in rough waters again because I consider it extremely unsafe, having almost drowned doing it in the past. To others, kayaking in a turbulent sea is ‘safe,’ even if they know someone who died from it. The risk of drowning — whatever that may be — is worth it for the thrill of kayaking through the waves.
The level of risk, or the amount of harm, to which one is exposed for an activity to be ‘safe’ depends on the individual. Tattoos are popular, but they hurt. Some people are interested in getting a tattoo but they know there is considerable pain involved, so it is not ‘safe’ or worth undertaking for them. If you have a moderate desire to get a tattoo, the pain probably isn’t worth it.
The public is inundated with propaganda to get vaccinated against SARS-CoV-2. As if that wasn’t enough, they are also mercilessly shamed and blatantly blackmailed into giving in. The collaborators in this effort chant that “The vaccines are safe!” But, as we have seen, ‘safe’ is relative. For someone to choose to pursue an action, the action must have an expected benefit and that benefit must be more important to the individual than the expected or potential negatives.
No one can determine for someone else that a medical treatment is safe. Only the person receiving the treatment stands to be harmed or benefited from it. No one has any right to decide for you if you should undergo a medical procedure, nor do they have any authority to decide for you that the procedure is ‘safe’ or ‘beneficial.’ There is only one person who is in a position to decide what is best for you – you!
There is nothing wrong with people offering their opinions on the safety of a treatment. From what I’ve read about SARS-CoV-2 ‘vaccines,’ they don’t appear to be safe or beneficial to anyone, but that is only my perspective. Get the shot if you want to, but please don’t let your government take away the rights of people who choose to remain non-genetically modified.
People should be free to express their opinions, including people representing pharmas or government agencies. But they are nothing more than opinions and claims. It is not possible to declare that a medical intervention is safe because safety is in the mind of each individual. It is the balance of expected rewards versus expected risks and how important those rewards and risks are to the individual that determine safety.
Safety is as much about expected benefits as it is about expected risks. An activity that could result in a severed limb would usually be thought of as unsafe, however, people have their limbs severed on purpose to prevent life-threatening gangrene. In that instance, it may be ‘unsafe’ not to lose a limb. As we’ll discuss below, not only do COVID vaccines have serious health risks, but very few people even have the potential to benefit from them.

U.S. lawyer Thomas Renz uncovered medical records from the U.S. Department of Defense in January 2022. Here is how the COVID vaccine rollout has affected the health of military personnel:
- 10x increase in neurological disease. Over 863,000 American military personnel now suffer from neurological disease thanks to the shots.
- 3x increase in miscarriages
- 60% increase in birth defects
- 4x increase in infertility across both genders
- 7x increase in multiple sclerosis
- 3x increase in cancer
- 71% of new cases and 60% of hospitalizations are in the fully vaccinated
FACTS ABOUT THE VAX
All of the coronavirus vaccines cause your body to produce a spike protein. The pharmas claim that the spike protein is non-toxic and stays in the injection site in your shoulder. However, scientists have recently learned that the protein is highly toxic and pervades all of your body’s tissues, including your brain.32 Paid propagandists continue to deny this, but according to Dr. Robert Malone, the inventor of mRNA vaccines, and many other renowned scientists, the evidence is now conclusive.¹ ² Many studies have shown that the vaccine opens the blood-brain barrier.23-31 The blood-brain barrier is the brain’s last line of protection from toxins and pathogens.
It is this cytotoxic spike protein that creates a danger of inflammation, bleeding, and blood clots throughout the body. The consequences of the clotting may be immediate or they may appear many years in the future. They may be dramatic, such as a heart attack, or they may be vague and difficult to pinpoint on the blood clot. Blood clots can cause countless symptoms and may be too small to show up on an MRI.
The spike protein appears to have particular affinity for reproductive organs in both males and females. In rodent studies in Japan of a COVID vaccine, there was a high concentration of the spike protein in the testes and ovaries. This has sparked concerns that the vaccines may cause infertility in humans. A June 2021 study published in the New England Journal of Medicine has found that over 80% of women in their first two trimesters of pregnancy had a miscarriage after receiving a COVID vaccine, confirming the infertility hypothesis. In 2022, an Australian doctor conducted his own study and discovered that vaccinated pregnant women miscarriage at a rate of 74% (the normal rate is 10-15%). Even more worrisome is that children of vaccinated parents are sometimes born with black eyes and display abnormal behavior and premature aging. Other newborns display the constant trembling that is common among adults who have been jabbed.
2 Essential Elements to Establish Safety
Although COVID pseudo-vaccines have alarming safety risks, there is a possibility that they may not produce as poor outcomes as the science would indicate. The risks for internal bleeding, blood clots, and antibody-dependent enhancement are based on scientific theory (and are beginning to rear their heads), but only time (and accurate data) will tell if those side effects are as sizable as scientists expect.
Two elements must be present to be able to assess the safety of a medical intervention. There must be a safety trial that lasts several years. Vaccine safety trials are generally 5-10 years minimum.³ There are many side effects that may not appear until years after the injection. One of the major health risks of COVID vaccines is antibody-dependent enhancement (ADE), also called pathogenic priming.
According to the scientists that have been raising awareness about ADE from COVID vaccines, it takes a few months to a few (eg. >5) years for it to cause severe illness. Neurological damage from the spike protein can also take many years to become apparent. Trials of COVID vaccines are under two years old. That is insufficient time to establish safety. There is no alternative to establishing vaccine safety short of a multi-year study. There are no shortcuts.
mRNA and DNA vaccines are both experimental and have unlimited potential to inflict harm. Even the inventor of mRNA vaccines, Dr. Robert Malone, considers the vaccines currently on the market for SARS-CoV-2 “experimental.” What kinds of things can go wrong with genetic engineering? The possibilities are endless, but, as an example, consider the following passage from a Johns Hopkins University Press publication.
Another well-known incident involving a human genetic experiment was an effort by French geneticists in 2000 to insert corrected genes into the bone marrow of babies born with a genetic condition that prevented them from developing an immune system. At first, the experiment seemed a success: the babies’ immune systems began to function perfectly, and the French doctors heralded this as the first complete gene therapy cure. Shortly afterward, however, three of the children developed leukemia, a form of cancer. It turned out that the retrovirus that the researchers had used to carry the corrected genes into the children’s DNA had unfortunately implanted itself too close to a cancer-causing gene, thereby activating it.
Maxwell Mehlman, Transhumanist Dreams and Dystopian Nightmares : The Promise and Peril of Genetic Engineering21
Graph: Vaccinology: Principles and Practice, John Marrow, 2012, p. 511.
The second essential element to establishing safety is accurate, honest data. Pharmas are known to fabricate data in their trials.18 19 20 Government agencies responsible for gathering information for the COVID vaccine program are utterly corrupt. In Canada, for instance, doctors try to report vaccine side effects and adverse reactions to the authorities only to be told that they are wrong — their patients must be ill due to some other reason.4 5 22 Canadian doctors are also publicly shamed and threatened with license revocation, and are sometimes fired for talking publicly about the side effects of COVID vaccines.
Contrary to what journalists tell us, clinical trials of COVID vaccines from the manufacturers themselves have not shown them to be safe. The Moderna and Pfizer trials showed equal numbers of deaths in the vaccine and placebo groups (which were of approximately equal size). However, it has been discovered that the numbers Pfizer reported to the FDA were 21 deaths in the vaccine group and 14 in the placebo group, owing to the higher incidence of fatal heart attacks. Note that the “95% effective” claim comes from there being two COVID deaths in the placebo group versus one in the vaccine group. That is the only basis for Pfizer absurd effectiveness claims.
The manufacturers own data, therefore, demonstrates that COVID vaccines are a net killer. This despite the fact that the trials reportedly had low integrity and the ‘safe and effective’ claim was made without raw data from the trial being made available. Without the data, they are marketing claims rather than a scientific ones, according to the BMJ’s Peter Doshi and Stanford Medicine’s Robert Kaplan.
Statistics on SARS-CoV-2 are consistently fraudulent. Reporting of adverse events and side effects from SARS-CoV-2 vaccines are equally corrupted. How, then, can we know how safe they are? We can’t. No matter how many years pass since the start of the vaccination program, it is impossible to make any statements about safety without an honest, uncorrupted mechanism for reporting, documenting, and publishing vaccination outcomes. Presently, none exists. The media is of no help, reporting that all deaths following vaccination are mere coincidences and slandering anyone who suggests otherwise.
No one can tell you that COVID vaccines, or any other radically novel medication, is safe without at least a few years of accurate follow-up data. Anyone you see on TV claiming that they are safe and recommending their use at this time is not being honest with you. They are either paid propagandists or lack the courage to express a counter-narrative view.

In England, all-cause mortality for non-seniors is 3x higher in the vaccinated as of Sept. 2021. READ MORE
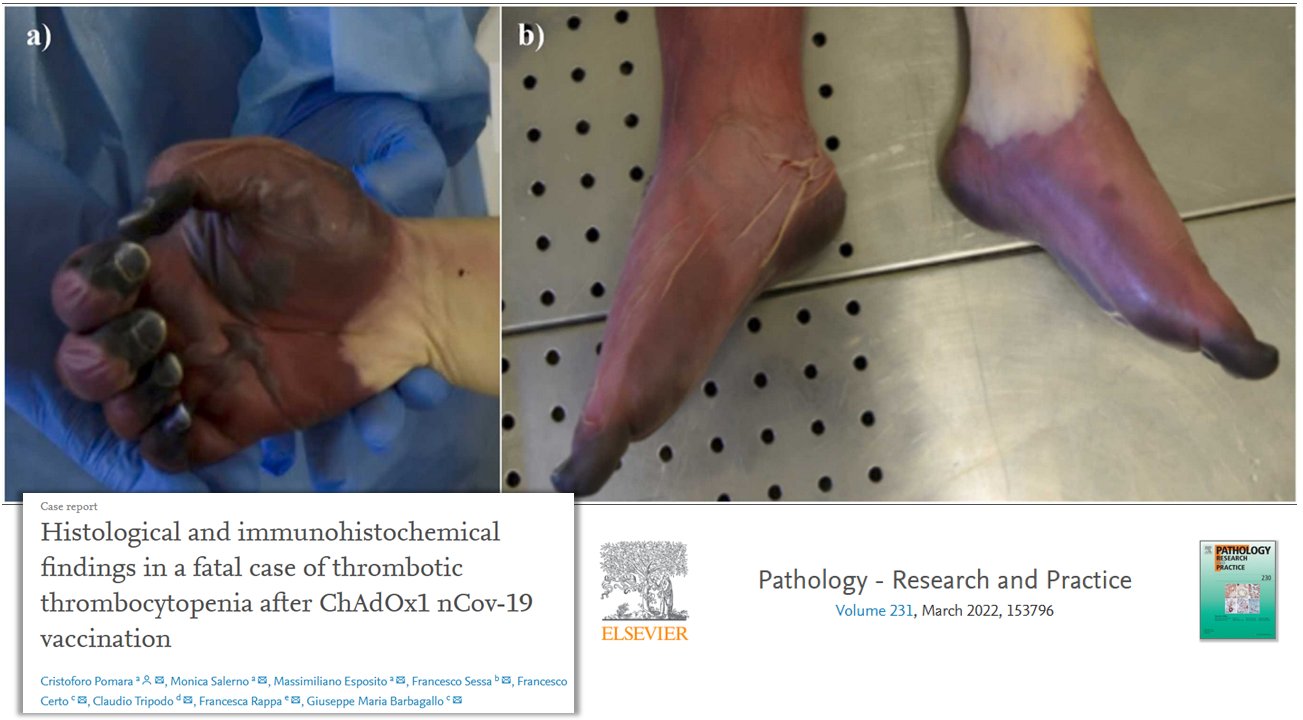
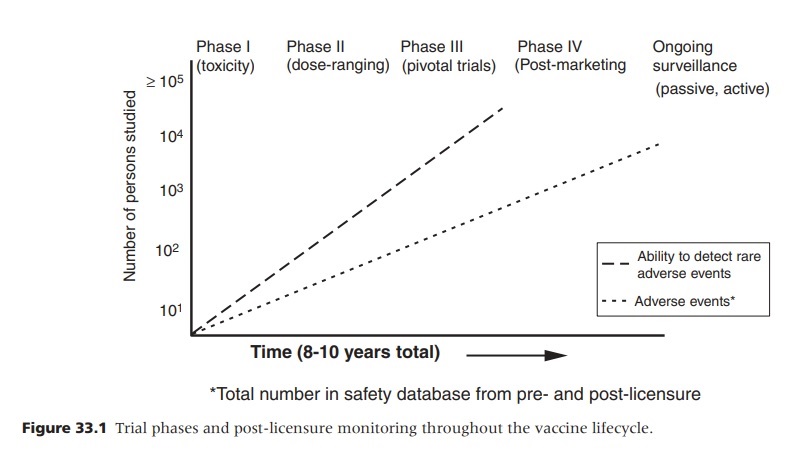
Young woman dies after developing blood clots from “safe” AstraZenica COVID vaccine. PAPER
Zero Benefit for People with Immunity
COVID pseudo-vaccines have very little potential benefit. There is only currently less than a 1% chance of any given person getting COVID-19 over a 12-month period.17 Therefore, for 99% of the population, there is no potential to benefit from the injections. Studies have found that up to 80% of people have pre-existing immunity to SARS-CoV-2 from exposure to similar pathogens.6 An April 2021 study at the University of British Columbia found that over 90-99% of people have SARS-CoV-2 antibodies. Thus, it could be that less than one in ten individuals are capable of ever benefiting from the pseudo-vaccines.
Some epidemiologists theorize that the true number of SARS-CoV-2 infections is much higher than the official case reports. John Ioannidis, Co-Director of the Meta-Research Innovation Center at Stanford, is one of the world’s pre-eminent infectious disease epidemiologists. In February 2021, he estimated that the number of people who had been infected by the Wuhan virus at that point was in the range of 1.5 to 2 billion.7 More recently, Dr. Sucharit Bhakdi, Germany’s most-cited microbiologist, has stated that herd immunity already exists for SARS-CoV-2 with a staggering 99% of people possessing the natural immunity to prevent the virus from going below the throat. (It is only fatal when it reaches the lungs.) Natural immunity from a SARS-CoV-2 infection is statistically perfect, and (as implicated by numerous studies) is probably permanent.
People with a prior SARS-CoV-2 infection (whether or not symptoms were present) are in the same boat as those with pre-existing immunity. They have absolutely nothing to gain from the COVID pseudo-vax. Nevertheless, the experimental gene therapy is being pushed onto them with equal vigor as the rest of society.
Systemic side effects in trials have occurred in over 80% of subjects.
⇑ Watch Now
99% CANNOT GET SEVERE COVID-19
In this riveting video from July 2021, Dr. Sucharit Bhakti reveals that 99% of people possess enough natural immunity to SARS-CoV-2 to prevent it from going below the throat, according to newly published studies. This is significant considering that the virus is only fatal if it infects the lungs. Below are the sources Bhakti used according to Oracle Films. Bhakti has also written a rebuttal to criticism of his presentation.
https://www.sciencedirect.com/science/article/pii/S2352396421002036 (v important DK)
https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0249499 v. imp. IgG IgA
response to mRNA vacc. +++
https://academic.oup.com/cid/advance-article/doi/10.1093/cid/ciab465/6279075 (key spike and IgG after vacc)
https://doi.org/10.1016/j.cell.2021.06.005 (third IgG response to vaccine paper)
One could argue that the annual rate of a COVID infection is irrelevant to vaccination — only the odds of getting COVID in one’s lifetime matter. I tend to disagree. I think that the annual rate matters most because COVID shots are meant to be annual and people can always begin taking them later.
Perhaps you are 55 years old and don’t think that the risks of the injections are worth mitigating the miniscule risk of death you have from COVID. However, you feel that once you hit 65, you will have a higher risk for a life-threatening coronavirus infection and want to have vaccine immunity at that age. Then just wait ten years to get vaccinated! If you don’t want the ‘vaccine’ now, you can always get it later! At two doses per year, you’d be sparing yourself 20 injections, along with the accompanying pain and illness. The decision on whether or not to get a COVID injection should only be based on the expected net benefit in the upcoming months.
Close to Zero Benefit for People without Immunity
It is widely known that COVID vaccines make you sick. 2.4+ billion doses have been administered so far. Most adults have been vaccinated in English countries, so if you haven’t had it, you’ve probably heard first hand the pain and sickness it causes. Systemic side effects in trials have occurred in over 80% of subjects.8 Many people who have had COVID then got vaccinated, report that the vaccination made them sicker than the virus. Since most people interested in vaccination are motivated to avoid dying or becoming critical ill from COVID, the odds of that happening in a 12-month period is a determining factor for getting vaccinated.
The odds of being hospitalized due to COVID in a 12-month period is very low. In Canada, it averages to 1 in 509 or 0.15% over the last 15 months.9 Thus, there is a 99.85% chance that a Canadian won’t need a COVID shot. There have been 3.7 million deaths attributed to COVID since the outbreak began 18 months ago. That is 205,555 deaths per month, or 2.46 million deaths per year. With a world population of 7.9 billion, that works out to a 0.03% chance of dying from COVID over the course of a year. Thus, if you only got vaccinated to prevent fatal COVID, there is a 99.97% (9,997 out of 10,000) chance that it was for nothing, even if the vaccine was effective.
There are two important caveats to the above figures, however. One is that most COVID statistics are grossly inflated. Actual deaths and hospitalizations could be a small fraction of official statistics. A second caveat is that historical data is not relevant. It is the expected odds of getting severe COVID-19 going forward that matter. With herd immunity approaching and safe, cheap medications available that both prevent cases and lower fatality rates by over 75%, historical data is hardly relevant.
Don’t the Elderly Need SARS-CoV-2 Vaccination?
Advanced age and pre-existing chronic illness are the primary risk factors for a life-threatening SARS-CoV-2 infection. The same could probably be said for all maladies, in fact. Assuming that you think that coronavirus vaccines are effective, you probably think that it is more important for the elderly and infirm to get them. That is certainly the prevailing sentiment. Who could argue that COVID vaccination is most important — and downright critical — for those at greatest risk for fatal COVID (eg. seniors who are immunocompromised or have chronic illness)?
Lots of people, evidently. Let’s start with the Norwegian Institute of Public Health. In January, they issued a statement that it is inappropriate to give a COVID vaccination to people who are old and in poor health. The institute cited both the increased risk of adverse reactions and the limited potential benefit due to being close to the end of one’s life. “For those with the most severe frailty, even relatively mild vaccine side effects can have serious consequences,” reported the institute. “For those who have a very short remaining life span anyway, the benefit of the vaccine may be marginal or irrelevant.”10
Filipino health officials have also argued against vaccination of those at highest risk of dying from COVID. Secretary of Health of the Philippines, Francisco Duque, stated that COVID vaccines are not advised for people who are very old or have a weak immune system.11 Duque’s sentiment was echoed by the Filipino Food and Drug Administration. The FDA of the Philippines has stated that Pfizer’s COVID vaccine is unadvised for the old and frail because of the heightened risk of adverse reactions.12
In December 2021, a Dutch statistical analysis assessed the hypothesis that COVID vaccination increases the risk of dying over three weeks following vaccination.33 The study discovered that people over 65 in Holland had a significantly higher risk of dying during the three week period, but people under 65 had no such risk. The authors recommended that COVID vaccinations be immediately halted due to the increased risk of dying following the injections among the elderly.
Ivermectin reduces COVID mortality by 96% when used as a prophylactic.
Leung Pak-yin, of Hong Kong’s COVID vaccination task force, has also advised against vaccinating seniors with poor health (the only demographic that dies from COVID). He doubts that they are strong enough to withstand the side effects of the injections and recommends protecting them from COVID using methods other than vaccination.13
Studies back these experts’ concerns of adverse reactions for the aged. Immunologist Dr. Theo Shetters has found that one in 800 Dutch seniors die from the COVID vaccine. An Israeli analysis found that their COVID vaccines have killed 40 times more elderly than would have died from COVID. The Vaccine Truth group recounts many studies and statistics, American and foreign, which put the death rate for COVID vaccines at 1-2 per 2000 persons. A large portion of these deaths are in the elderly.
Australian tennis star Pat Cash describing a typical response of a senior to a SARS-CoV-2 vaccine.
Not only are COVID pseudo-vaccines unacceptably dangerous for the elderly, they may also be much less effective. The immune system wanes in old age, a phenomenon called immunosenescence. That is a major reason why SARS-CoV-2 and the flu kill the elderly almost exclusively. The efficacy rates you have heard about for COVID vaccines are not age-specific. They are the average across all ages of subjects.
As a generalization, in people of advanced age — over 75, for instance — immunity (including post-vaccination immunity) is substantially lower than for younger cohorts. Also, only healthy people were included in the vaccine trials. Vaccine efficacy ratings are thus unknown for those in poor health and for those in the upper age range. We can expect them to be far lower in those demographics. Efficacy of flu vaccines is 56% lower in seniors than in younger ages.15 A similar age correlation of COVID shots would put them below the CDC’s 50% minimum effectiveness cut-off.
Manufacturers of COVID pseudo-vaccines claim that they are almost as effective in seniors as non-seniors. Pfizer and Moderna actually put the senior efficacy rate at 94%, only 1% lower than the all-age average. How impressive. If you believe the pharmaceuticals, why are you even reading this website? Just take the drug and neglect your natural immune system like they tell you to. I, for one, find it very hard to believe that efficacy in seniors is close to that of younger people since it defies everything that I’ve read about vaccination and immunity in seniors. I think they are hiding the truth. In July 2021, Sarah Gilbert, head researcher for the Oxford-AstraZeneca COVID vaccine, admitted that people with compromised health “just don’t respond to a vaccine.”
UK government data shows that COVID-vaccinated seniors have six times the all-cause death rate as unvaccinated seniors, June 2022. FULL VIDEO
Even if a vaccine (for coronavirus or something else) was safe and effective, it still would be useless to employ during a pandemic because 1) vaccines don’t work in the one group that is at risk for severe illness in a pandemic — the old and unhealthy, and 2) for other groups, it would take at least 2 years to get safety data, at which time a real pandemic would have been long over. So argues Dr. Mike Yeadon, May 2022.

Yeadon expresses his view that early treatment is preferable to COVID vaccination for every age group in this social media post, August 19, 2021.
Read also his 7 Reasons why the COVID vaccines and vaccine mandates should not be approved post.

UN POSITION PRIOR TO THE TERROR
“Gene editing has opened a Pandora’s Box. While it presents great hopes for curing disease and eliminating hunger, gene editing is still imprecise, which could lead to inadvertent and undesirable changes to a genome. There are also concerns regarding the unknown, long-term safety of gene editing.”
Playing with genes: The good, the bad and the ugly, United Nations, 2019
« Read the Document
Safety is Relative to the Alternatives
The lockdown-vaccine conspirators will never tell you that there are safer ways to lower the incidence of critical COVID-19 than vaccines. The COVID-19 Early Treatment Tracker currently lists 13 old medications and supplements for which studies show significantly lower SARS-CoV-2 illness and mortality. I highly recommend you keep track of the tracker.
Ivermectin and HCQ each have countless studies demonstrating their effectiveness. When administered early, they reduce mortality by 81% and 75%, respectively.15 Amazingly, those aren’t even the most effective treatments! If vax advocates were not completely corrupt, they wouldn’t be denying the effectiveness of these treatments. Many governments, including the U.S., actually have forbidden these harmless life-saving treatments in an effort to maximize COVID deaths. In Queensland, Australia, treating COVID is a crime. A doctor can go to prison for prescribing medications for COVID.
The fact that there are treatments for COVID that lower mortality in the alleged range of vaccine effectiveness changes everything. These are safe medications that have been around for decades and are being repurposed for SARS-CoV-2. They make vaccination utterly futile. They can even reduce COVID in the population without waiting for people to fall ill. Ivermectin reduces COVID mortality by 96% when used as a prophylactic. Unlike COVID pseudo-vaccines, these time-tested medications do not have serious side effects.
Poor Integrity of the Pseudo-Vaccine Conspirators
The agents pushing COVID vaccines know that they are dangerous and their efficacy is unknown. This is apparent by the fact that the injections are primarily promoted using lies and propaganda. Notably, everyone promoting the treatment denies that they are missing critical safeguards discussed in The Vaccine Agenda. They also make claims that are impossible to back up, such as the vaccines being safe — that can only be determined from years of accurate data, as explained above.
If COVID “vaccination” was really a desirable treatment, you wouldn’t need to coerce people into getting them. There are many lotteries for vaccines, tempting people with millions of dollars to submit to vaccination. Many countries are currently blackmailing people into getting vaccinated, such as forcing people not vaccinated to wear masks.
In Canada, many provinces have a minimum level of vaccination before easing restrictions, usually 70%.16 That means that even when deaths approach zero due to herd immunity and effective treatment, the province will still be a veritable prison. Clearly, the rulers of the provinces are waging a perverse war against their own people. Public health has nothing to do with their actions.
Nearly every form of lockdown propaganda mentioned in Mind Control is also used to promote uptake of the pseudo-vaccines. Celebrities are filmed while getting injected. People refusing the injection are mercilessly bullied and shamed publicly. The conspirators claim that only stupid or crazy people would turn down the injections. Doctors are fired for discussing the vaccines critically.
Governments are manipulating healthcare data to hide the epidemic of adverse reactions from COVID vaccines. In Canada, for instance, the government won’t even accept reports of the reactions. The media won’t report on the issue except to say that no one ever dies from COVID vaccines. If the treatment was actually safe, there wouldn’t be anything to hide, would there?
Anyone harking SARS-CoV-2 “vaccines” as safe is a liar with no scientific credibility. The most favorable statement that could be made about the pseudo-vaccines is that the rate of people who will succumb to immunity-destroying pathogenic priming or the poisonous spike protein has yet to be discovered.
Relative safety for a radical gene editing technology can only be gleaned from a decade or more of accurate data collection (including for alternative treatments). In over 30 years, this technology has never passed human or animal safety trials. The perpetual lying and bullying by the cheerleaders of this therapy is testament to their lack of moral or scientific authority. Of course, the advocates for COVID gene therapy are the same false public health prophets that brought us universal home incarceration and respiratory suppression to save us from Armageddon. They have all the concern for public wellbeing as Xi Jinping, the pioneer of lockdowns.
While no one can legitimately claim that SARS-CoV-2 vaccines are safe, I can say, without reservation, that they are unsafe. I have proven that they have nightmarish health risks and extremely high rates of side effects. Furthermore, there is no need for them, particularly when you consider that there are safe, effective treatments for COVID going unused. ‘Safety’ means the absence of risk. This treatment has extremely high risks with minimal benefits.
Be that as it may, it is up to each person to determine as an individual if the benefits outweigh the risks for him/herself. That requires informed consent and a halt to the coercion and blackmail. Everyone should have all of their rights reinstated immediately, vaccinated or not. Censorship must end and its perpetrators imprisoned.